Elevate’s Ankle Sprain Rehab
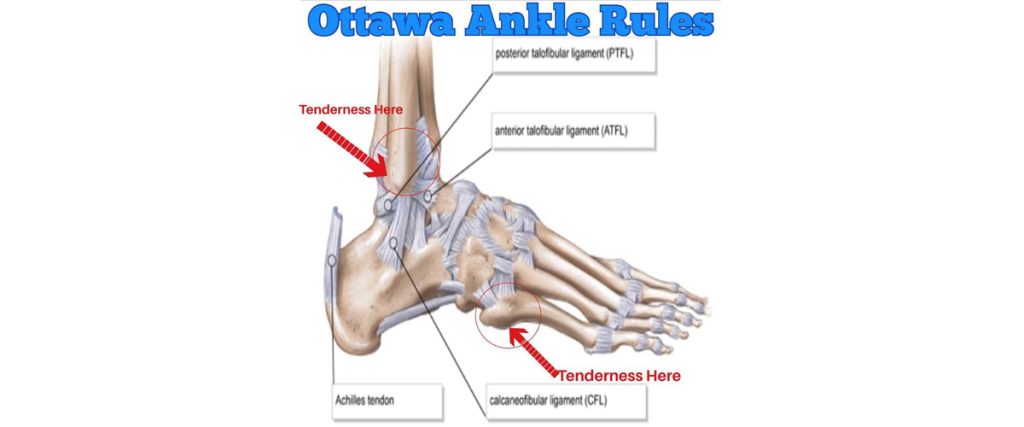
Sometimes it’s difficult to know if you’ve rolled your ankle or done something more that may require an x-ray. The Ottawa Ankle Rules help us decide whether or not an x-ray is warranted: Unable to put any weight on your injured side for 4 steps Tenderness at the base of your 5th toe. Tenderness 6 cm up from your ankle bone. If you have any of the above-mentioned rules, then you should get an x-ray to rule out a fracture. Lateral Ankle Sprains can vary in their severity. Clinically, ankle sprains are generally classified into three groups: Grade 1: A stretch of the ligament that does not result in a tear. There is minimal swelling and tenderness, mild or no loss of function, and no mechanical instability of the ankle. Generally associated with strain to the ATFL. Grade 2: A partial tear of the ligament with moderate pain, tenderness, and swelling. There is some loss of function and presence of mild to moderate mechanical instability. Generally associated with strain to both the ATFL and CFL. Grade 3: A complete tear of the ligament with significant bruising, swelling, and tenderness. There may be an inability to bear weight on that foot, and there is significant instability of the ankle. Generally associated with strain to the ATFL, CFL, and potentially the PTFL as well. There may be swelling, bruising, and tenderness in your foot and ankle. It is important to note that the amount of swelling and bruising is not always indicative of severity of tissue damage. The best time to have a physical examination by your Physical Therapist is 4-5 days after your injury. After an ankle sprain it is important to work on ankle mobility, motor control, and balance. The following exercises show a few examples of some exercises used to address those impairments. 1.Ankle CARs (Controlled Articular Rotations) – helps to regain mobility and useful as an assessment of motor control 2.CRAs Correctives – if you find an area of movement during your CARs that is more challenging or in uncontrolled (might be shaky or not a smooth path of movement), then you can work in that uncontrolled range to help improve your control over that particular range 3.Single Leg Balance – the video shows progressively more challenging ways of working on single leg balance. If you are in a lot of pain still and cannot bear your full weight on your injured side, you can do these exercises on your other side since there is a known cross-over effect for these exercises (training one side of the body will also have a training effect on the other side of the body) 4.Multi-directional reach – this works on your single leg stability in multiple planes of movement In order to promote healing and help reduce the risk of future injury, it is important to progressively overload the tissues that support the ankle in order to create adaptation. The exercises in this video demonstrate a few ways that you can target loading of ankle inversion. Medial/Lateral Lunge Three Way Step Down Cross-Over Step Up Single Leg Medial/Lateral Reaches Single Leg RDL Single Leg Airplane With Rotations Single Leg Golfer RDL’s Single Leg Lateral Med Ball Toss You can gradually add weight to these to make them more challenging.


