Is Your Athlete At Risk?
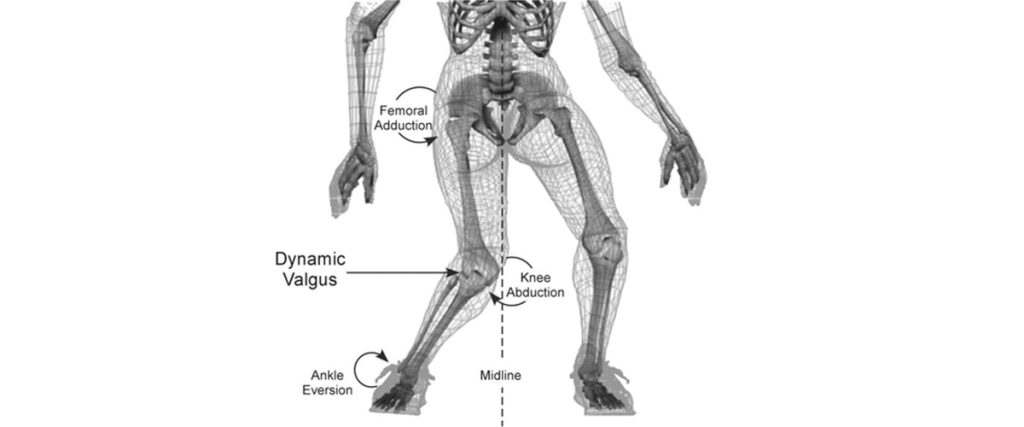
KNEE INJURIES – IS YOUR ATHLETE AT RISK? THREE EASY TESTS! Movement Performance Assessments are a key measure to reveal young athletes’ risks for injury, learn what to do to bulletproof against them, and increase their odds of staying healthy and playing great during the season. PREVENTABLE KNEE INJURIES The knee is the most commonly injured joint in adolescent athletes. Lost play time, not to mention pain, rehab, and potential long-term disability are common realities with knee injuries. Some of the more common ones are patellofemoral pain (“runner’s knee”), IT Band Syndrome, and patellar tendinitis (“jumper’s knee”), ligament sprains, and meniscus tears. Two additional injuries common in the skeletally immature are Osgood Schlatter’s disease and osteochondritis dessicans (OCD). The less common (yet numbers are rising in our youth athletes) and more catastrophic injury is the ACL (anterior cruciate ligament) tear. Seventy percent of ACL tears are non-contact injuries that occur during movements like cutting, twisting, decelerating, and landing from a jump, without making any contact with another player, in sports like soccer, basketball, lacrosse, football, volleyball, and tennis. It’s important to note too that there is a four to six-fold greater incidence in female athletes compared to males playing the same landing and cutting sports. Current research by many including Dr. Christopher Powers, Professor of Biokinesiology & Physical Therapy at USC, has revealed a number of modifiable risk factors associated with knee injuries, including the devastating ACL tear, i.e. weakness and poor control of the trunk, pelvis, hips, and knees, and poor body alignment during movement. Dr. Timothy Hewett of The Mayo Clinic Orthopedic Biomechanics Lab describes these modifiable risk factors as: ligament dominance; quadriceps dominance; leg dominance; and trunk dominance, all of which can be changed to improve the odds of avoiding an injury. These are preventable injuries. But how? TEST to uncover deficiencies associated with injury Get key muscles strong Improve high-level balance Train strength & balance with optimal movement Incorporate into sport-specific movement (“neuromuscular control”) during warm-up and training Good movers become better athletes and have fewer injuries. TESTING There are numerous tests with complex scoring systems and criteria that we run for individuals and teams both in the clinic and on the field. We use the latest evidence in testing and advanced technology to determine an athlete’s risk profile, we score the tests individually and look at them collectively to determine an athlete’s level of risk for injury. Then we teach what to do. If an athlete has been injured, we use these tests to determine return-to-sport readiness as well. But here’s the good news… A few simple tests can detect key risk factors associated with knee pain and injuries, including the devastating ACL tear. Step-Down Test 10 Second Tuck Jump Drop Jump Test The Step-Down Test is a low impact, basic indicator of an athlete’s single leg, dynamic strength, control, and preferred movement patterns. What to look for that reveals greater risk for injury: Excessive leaning of the trunk (poor trunk control) Excessive drop of one side of the pelvis toward the ground (poor pelvic control) (#1 and #2 can often go hand-in-hand, as in the video, and even though the knee may not appear to drop inward (valgus angle), the combination of the two can create a valgus torque at the knee.) Rotating the thigh and the knee collapsing inward (dynamic valgus/poor hip utilization) Upright trunk (quadriceps dominance / poor hip utilization) The 10 Second Tuck Jump, formalized and studied by Dr. Gregory D. Myer, sports biomechanist at the Cincinnati Children’s Hospital Sports Medicine Biodynamics Center, is a ‘double leg ballistic/plyometric’ activity (jumping on both legs), increasing the demand to the system compared to the Step-Down Test. It’s a great one to do on the field because it doesn’t require any equipment. Have your athlete try it. Take a video and use slow motion if possible. Jump for 10 seconds, trying to lift knees to hip height and trying to land on the same spot, without pausing. While watching the video, see if your athlete’s knees collapse inward (dynamic valgus), like the knees are kissing, as the feet hit or push off from the ground. If they do, like the young woman in the video, your athlete is at greater risk. If your athlete looks more like the young man in the video, the chances of injury are lower. We actually score 10 criteria in this test, but here are five easy things to pick out that will give you insight into risk for injury: Knees collapsing inward / dynamic valgus Knees uneven and not reaching hip height Stiff knee landing Landing on one leg before the other Not remaining in the same ‘footprint’ throughout the 10 seconds The Drop Jump Test “before” video demonstrates “dynamic valgus” (inward collapse of the knees) in a volleyball athlete. It’s one movement pattern associated with knee pain and injuries. The “after” video demonstrates this same athlete after some strength, balance and movement training, using a band above the knees to cue and facilitate her gluteal muscles to control the movement and protect her knees. Dynamic valgus, combined with poor shock absorption and poor trunk control during cutting, twisting or landing can overload the ACL in a split second. Wear and tear from dynamic valgus during daily activities and sports is also associated with the more common knee injuries mentioned. COMPREHENSIVE MOVEMENT PERFORMANCE TESTING Try these three tests at home or on the field and see how you do. Come in to do a comprehensive Movement Performance Assessment of 8 tests, including running and cutting sport-specific tests with video analysis with our PT team specializing in sports and biomechanics and learn what to do. Taking time to learn which modifiable risk factors your athlete demonstrates and what to do about them will help your athlete avoid injury, achieve top performance, and STAY IN THE GAME.